Burn Injury as a Complex System
Burns are characterised by a massive and prolonged acute inflammation, which persists for up to months after the initial trauma1. Due to the persistence of the inflammatory process2, predicting the dynamics of wound healing can be particularly challenging after burn injury3.
From the molecular level to organs, the body operates as nested complex systems: biochemical interactions govern protein synthesis and cell signalling; cells divide, communicate, and perform metabolic activities; tissues organise into organs; and organs cooperate to maintain homeostasis. In severe burn injuries, this layered balance is disrupted simultaneously across all levels, triggering acute kidney failure, hypermetabolism, and prolonged immune dysregulation.
Understanding this complex system through a computational lens allows us to explore phenomena from molecular to systemic scales, design treatment strategies, and predict the development of the healing process2.
Cellular and Molecular Interactions
The Inflammatory Cascade
In burn wounds, cellular and molecular interactions coordinate a dynamic healing process beginning with acute inflammation and complement activation. Necrotic tissue releases damage-associated molecular patterns (DAMPs) such as HMGB1 and heat shock proteins, which activate pattern-recognition receptors (TLR4, NLRP3) on resident immune cells. This triggers an immediate immune reaction, releasing pro-inflammatory cytokines including TNF-alpha, IL-1beta, and IL-6, alongside activation of all three complement pathways (classical, lectin, alternative). A recent systematic review and meta-analysis of 110 studies confirmed significant post-burn elevations in C3a, C3b, C5a, factor B, and the membrane attack complex (Mulder et al., Front Immunol, 2026). C5a in particular acts as one of the most potent chemoattractants known, recruiting neutrophils and macrophages to the injury site at nanomolar concentrations.
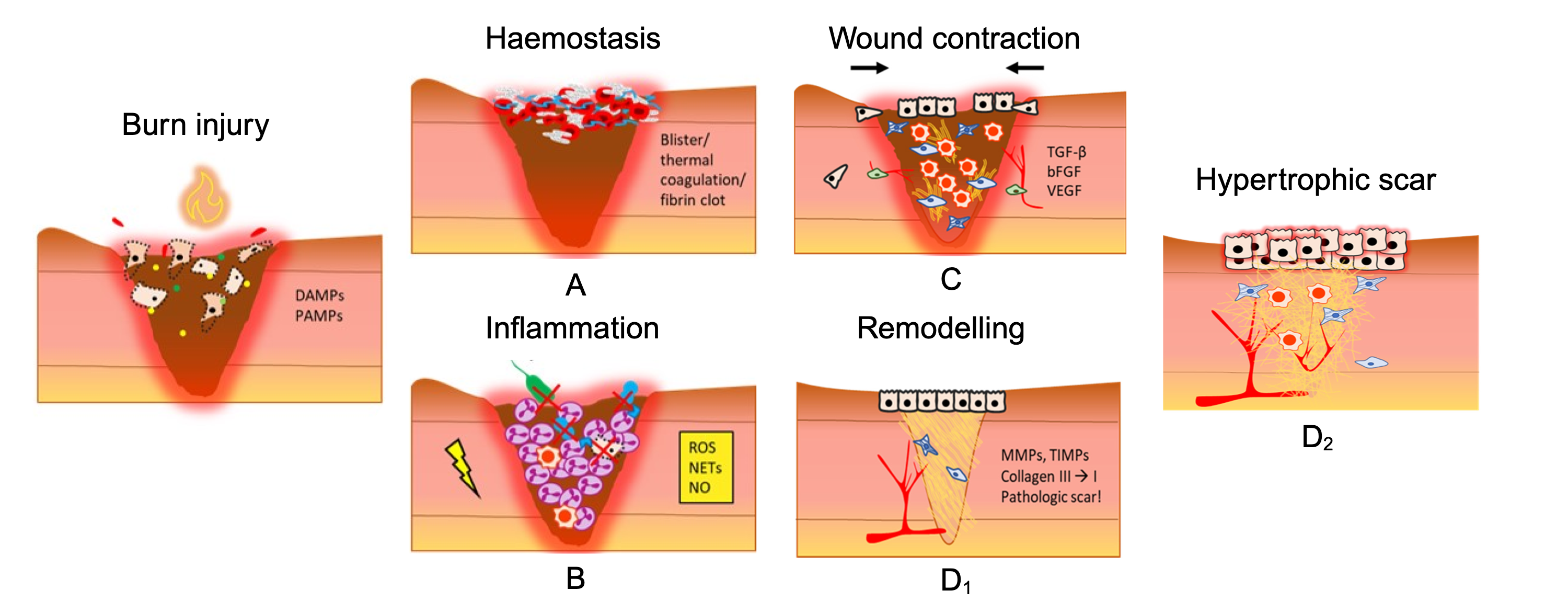
Wound contraction during the proliferative phase involves myofibroblasts generating contractile forces to pull wound edges closed, while collagen types I, III, and IV provide structural ECM support.
The remodeling phase brings MMP/TIMP-regulated ECM turnover. When dysregulated, excess deposition leads to hypertrophic scars and keloids, a major clinical challenge in burn care.
Excessive inflammation not only exacerbates local tissue damage but drives systemic effects: hypermetabolism, organ dysfunction, and prolonged hospitalisation.
Dynamics of the Immune Response
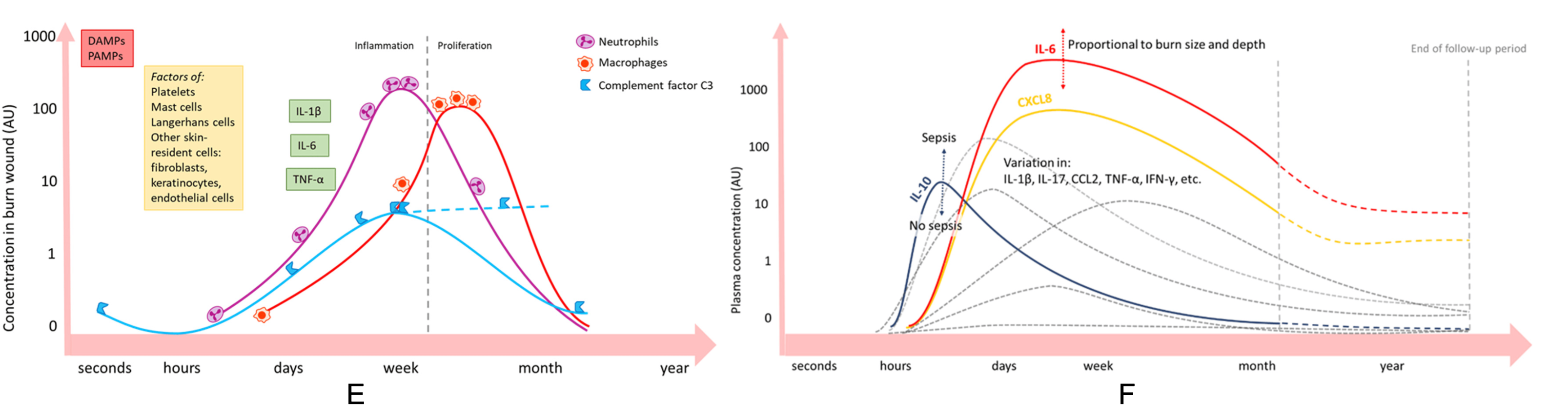
These immune cells, recruited via complement-driven chemotaxis, play critical roles through phagocytosis, reactive oxygen species (ROS) release, and secretion of pro-inflammatory mediators. Understanding the interplay between dysregulated complement activation, acute inflammation, and wound healing is essential for targeting interventions at the right phase and mechanism.
Computational Modeling Approach
Computational modeling has been applied to biological systems for decades, but its use in burn injury remains limited compared to other fields such as oncology or cardiovascular medicine. For burn injury, these models draw from clinical observations, experimental studies, and imaging data to simulate the progression of healing and predict physiological outcomes. Recent work has demonstrated that neural network surrogates can accelerate finite element simulations of post-burn contraction by several orders of magnitude (Egberts et al., Front Appl Math Stat, 2023; Husanovic et al., Clin Biomech, 2025), suggesting that real-time clinical decision support may become computationally feasible.
The main focus for COMBI is to facilitate the study of the underlying mechanisms of inflammation, wound healing, and scar formation, enabling insights into the molecular and cellular origin of complications arising from burn injury. COMBI distinguishes itself from existing wound healing models by integrating three spatial scales (molecular, cellular, tissue) within a single framework calibrated specifically to burn pathophysiology rather than general wound healing.
Each model in COMBI targets a specific phase of wound healing, building toward an integrated in silico clinical trial tool for treatment optimisation.
Agent-based ODE systems Spatio-temporal Multi-scaleModeling Roadmap
Each phase of wound healing presents distinct computational challenges. The COMBI roadmap sequences these into five interlocking modeling objectives:
Complement activation without adaptive immune response. First-responder dynamics.
Full-window inflammatory response with adaptive immune components. See MAP4b publication →
Myofibroblast activity and collagen deposition in 2D and 3D. MechaProlif publication (IEEE BIBM 2023)
Clinical scar patterning and in silico replication of hypertrophic scarring dynamics.
Implementing treatment approaches and finalising the tool for clinical decision aid.
Explore the Models
MechaProlif Model
Myofibroblast and fibroblast dynamics during the proliferative phase. Explore the model and its parameter scenarios.
Explore model →
Angiogenesis Model
Spatio-temporal model of endothelial cell dynamics and blood vessel regrowth in a burn wound patch.
Explore model →